3D bioprinting is a specialised branch of additive manufacturing that deposits living cells, bioactive molecules, and biomaterial scaffolds layer by layer to engineer functional human tissues. While conventional 3D printing builds objects from plastics, metals, even concrete for consumer and industrial use, bioprinting works within strict biological constraints (temperature, pH, sterility, and cell viability) to create tissues and organs for medical research and, increasingly, clinical transplantation. In October 2025, the world’s first 3D-bioprinted cornea was successfully transplanted into a legally blind patient, marking a milestone that I believe will be looked back on as the moment bioprinting moved from laboratory promise to clinical reality.
Through this article I want to explain what sets 3D printing and 3D bioprinting apart, how they remain connected through shared engineering principles, and what these technologies can realistically achieve in 2026 and in the coming future.
How 3D Bioprinting Grew Out of 3D Printing
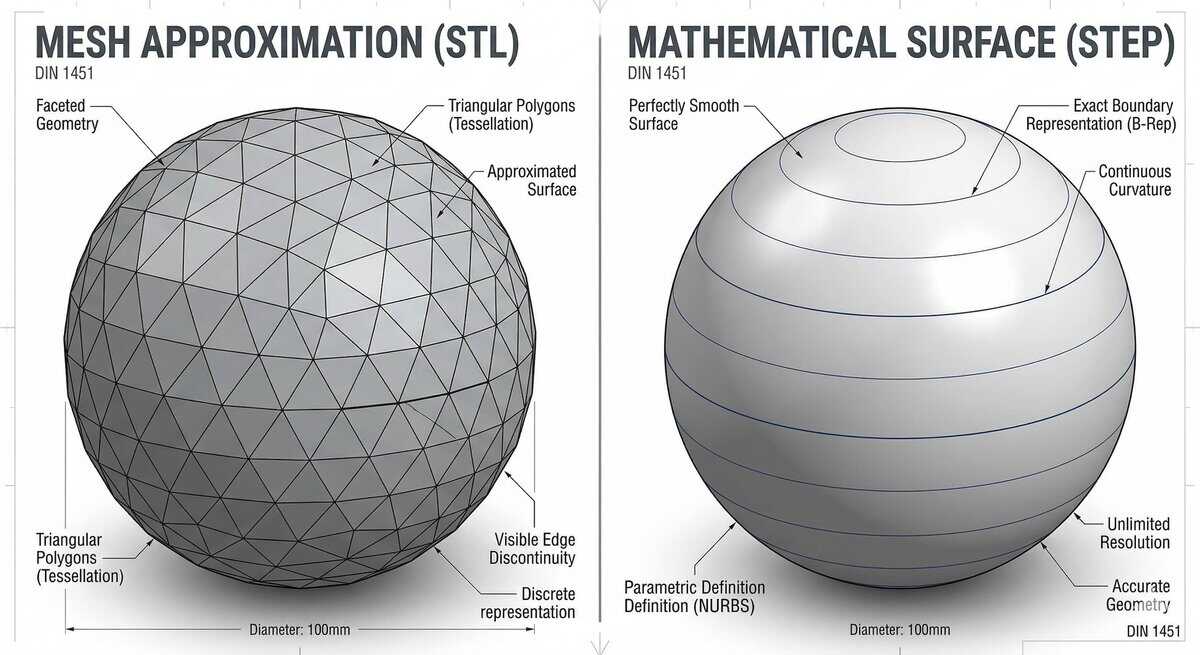
3D Bioprinting did not emerge in isolation. It inherits its core mechanics, such as layer-by-layer build logic, CAD-to-slice workflow, and most directly the nozzle-and-extrusion print-head, from two foundational breakthroughs in the history of 3D printing during the 1980s. Charles W. Hull’s 1984 stereolithography patent established the layer-by-layer principle and the STL file format that bioprinting still uses to translate CAD geometry into printable slices. Four years later, S. Scott Crump’s invention of Fused Deposition Modelling (FDM) introduced the heated-nozzle extrusion architecture that most of today’s extrusion-based bioprinters now use, with living cells in a hydrogel carrier replacing the molten plastic.
The conceptual leap from printing inert materials to printing living cells traces back to Robert J. Klebe’s 1988 “cytoscribing” experiment, where he used an inkjet printer to deposit biological products. The truly groundbreaking moment came in 2003 when Thomas Boland at Clemson University modified a standard HP inkjet printer by replacing the ink with suspensions of living cells. His team demonstrated viable cellular patterns with approximately 75% post-printing cell viability, proving that printer technology could handle biological material without destroying it.
From that point, 3D bioprinting accelerated rapidly. Organovo, founded in 2007, produced the first fully cellular bioprinted blood vessel in 2010. Anthony Atala’s team at the Wake Forest Institute for Regenerative Medicine demonstrated human-scale bioprinted tissues in 2016. And Adam Feinberg’s FRESH (Freeform Reversible Embedding of Suspended Hydrogels) technique, refined in 2019, achieved 20-micrometre collagen filament resolution by printing soft hydrogels inside a gelatin support bath, opening the door to printing structures as complex as a miniature human heart.
I have been tracking these developments for years, and what strikes me most is how each breakthrough built directly on conventional 3D printing principles. The layer-by-layer logic, the computer-aided design workflow, the slicing software: all of it carries over. What changes entirely in 3D bioprinting is what you print with and why.
What Is Regular 3D Printing? A Brief Recap
If you are new to the field, here is a quick overview (you can skip this section if you already know how 3D printing works). 3D printing, also called additive manufacturing, builds three-dimensional objects by adding material layer by layer, guided by a digital CAD model. It stands in contrast to subtractive methods like CNC machining, which cut material away from a solid block.
The seven primary types of additive manufacturing include:
- Fused Deposition Modelling (FDM/FFF): Extrudes thermoplastic filament (PLA, ABS, PEEK) through a heated nozzle. The most widely used desktop technology, known for affordability and ease of use.
- Stereolithography (SLA): Uses a UV laser to cure liquid photopolymer resin, achieving layer resolutions as fine as 25 microns.
- Selective Laser Sintering (SLS): Fuses polymer powder particles using a CO₂ laser, producing parts with near-isotropic mechanical properties.
- Digital Light Processing (DLP): Projects entire layer images simultaneously, curing each layer in seconds regardless of geometric complexity.
- Material Jetting: Deposits droplets of photopolymer achieving the finest conventional resolution at 14–16 micrometre layer heights.
- Binder Jetting: Selectively deposits a liquid binding agent onto a powder bed.
- Directed Energy Deposition (DED): Uses focused thermal energy to fuse metal wire or powder as it is deposited.
These technologies process inert materials, including thermoplastics, metals, ceramics, and photopolymers, at temperatures ranging from 180°C for PLA to over 1,500°C for titanium alloys. The primary design constraints are mechanical: tensile strength, dimensional accuracy, surface finish, and thermal management.
What Is 3D Bioprinting?
3D bioprinting is the computer-controlled, layer-by-layer deposition of living cells, biomaterials (called bioinks), and bioactive molecules to fabricate three-dimensional tissue and organ constructs that mimic native human physiology.
The critical distinction from conventional 3D printing is this: living cells must be present during the printing process itself. This separates true bioprinting from the 3D printing of acellular medical devices, such as titanium hip implants or polymer surgical guides, which use standard additive manufacturing techniques despite their medical end-use.
Technically, 3D bioprinting is defined as the fabrication of complex three-dimensional functional living tissues from biocompatible materials, living cells, and supporting components. There are multiple types of biocompatible materials used for bioprinting and we will talk about it later but it is important to note that all are not the same. For example, the terms bioink and biomaterial ink are often used interchangeably, but they refer to different things.
A bioink is a formulation that contains living cells and is processed by the bioprinter, while a biomaterial ink is a cell-free formulation where cells are only seeded after printing. This distinction has direct regulatory and manufacturing implications. Bioinks face much narrower processing windows: temperature between 4–37°C, pH between 6.5–7.4, shear stress below 5 kPa, and sterile conditions throughout.
3D Printing vs 3D Bioprinting: Key Differences

Conventional 3D printing builds objects from inert materials like plastics, metals, and resins. 3D bioprinting deposits living cells, bioinks, and bioactive molecules to create functional tissue constructs. The key differentiator is the presence of living cells during printing, which constrains temperature, sterility, and mechanical forces.
Here is a structured comparison across five critical parameters:
| Parameter | Conventional 3D Printing | 3D Bioprinting |
| Materials | Inert thermoplastics (PLA, ABS, PEEK), metal powders, photopolymer resins, ceramics | Cell-laden hydrogels (alginate, GelMA, collagen), decellularised Extracellular Matrix (ECM), bioactive molecules with living human cells |
| Purpose | Rapid prototyping, industrial tooling, consumer products, non-living medical implants | Tissue engineering, organ scaffolds, drug testing, disease modelling, personalised medicine |
| Equipment | High-energy systems: heated nozzles (180–420°C), lasers, heated beds, inert gas chambers | Low-energy sterile systems: temperature-controlled extruders (4–37°C), HEPA-filtered enclosures, UV/visible-light curing |
| Precision | Dimensional accuracy (±0.1–0.3 mm), thermal management, mechanical strength optimisation | Cell viability preservation, shear stress management below 5 kPa, biochemical gradient control |
| Post-Processing | Mechanical: support removal, sanding, heat treatment, sintering at 900–1200°C | Biological: ionic/UV crosslinking, bioreactor incubation (days to weeks), tissue maturation with perfusion |
The fundamental difference is that conventional 3D printing optimises for structural permanence and mechanical strength, operating within a parameter space governed by thermodynamics. 3D Bioprinting operates within a highly constrained “biofabrication window” where the primary objective is maintaining cellular homeostasis, which involves keeping cells alive, healthy, and functional throughout the entire process.
From my experience covering both fields, I have found that the easiest way to grasp this difference is to think about temperature. A standard FDM printer melts plastic at 200°C or more. A bioprinter must keep its payload below 37°C, human body temperature, or risk killing the very cells it is trying to arrange. That single constraint changes everything about how the machine, the materials, and the workflow are designed.
How 3D Bioprinting Works: The Three Stages

3D Bioprinting works in three stages. First, a digital model of the target tissue is prepared and cells are grown in the lab and mixed into a printable bioink. Second, the bioprinter deposits that bioink layer by layer to build the physical structure. Third, the printed construct is matured in a bioreactor until the cells organise themselves into functional living tissue.
Stage 1: Pre-Bioprinting
Before anything is printed, two things have to happen in parallel. On the digital side, doctors take a scan of the patient, usually an MRI or CT, and convert it into a 3D model the printer can understand. Medical imaging software such as Materialise Mimics or the open-source 3D Slicer handles this conversion, and the model is then sliced into thin horizontal layers that tell the printer exactly where to deposit material.
On the biological side, the cells that will populate the final tissue are harvested (often from the patient’s own body), grown in a lab over one to four weeks until there are enough of them, and then mixed into the bioink. For most extrusion-based printing, the final mixture contains one to ten million cells in every millilitre.
Stage 2: Bioprinting
This is the printing step itself. The cell-loaded bioink is deposited layer by layer onto a sterile surface, with the printer head moving under computer control in the same way a desktop 3D printer moves. What makes it harder than ordinary 3D printing is that every parameter has to be tuned to keep the cells alive. Push the bioink too hard and the shear forces damage them. Print too cold or too warm and the hydrogel either clogs the nozzle or collapses. Use too fine a nozzle and you get better resolution but more cell death.
For the softest materials (the ones that would normally slump into a puddle the moment they leave the nozzle), a technique called FRESH prints the structure inside a supporting gel bath that holds everything in place until the material sets.
Stage 3: Post-Bioprinting
This is where most people are surprised to learn that the printed object is not yet a functional tissue. It is only a template: a scaffold holding cells in the right spatial arrangement. Becoming actual living tissue takes weeks of additional work.
First, the printed structure is stabilised through a process called crosslinking, which locks the hydrogel into its final shape using light, chemicals, or enzymes depending on the material. Then the construct is moved into a bioreactor, which is essentially an incubator that feeds the cells a continuous stream of nutrients and applies the physical forces the tissue would experience inside a real body. Over time, the cells respond to these cues by organising themselves into functional tissue, forming connections, aligning in the right directions, and taking on the biological behaviour of the organ they are meant to replace.
How long this takes depends on what is being grown. Blood vessels are relatively quick at one to two weeks. Cartilage needs two to four weeks. Bone, which has to mineralise into a hard structure, can take up to eight weeks.
For anyone studying or entering the field, it is worth remembering that the post-bioprinting phase is where the real biology happens. Printing is the starting line, not the finish line.
3D Bioprinting Technologies: Four Modalities

3D Bioprinting technologies in 2026 fall into four primary modalities: extrusion-based, inkjet (droplet-based), laser-assisted (LAB/LIFT), and SLA/DLP. Each differs in how it deposits or shapes cell-laden bioinks, making them suitable for specific viscosity ranges, resolution requirements, and cell types. These distinctions determine their applications across research, drug development, and tissue engineering, with each modality optimised for a particular balance of precision, scalability, and cell viability.
Extrusion-Based Bioprinting
The most widely used modality. A pneumatic, piston-driven, or screw-driven system continuously dispenses bioink through a micro-nozzle. It handles the widest viscosity range and supports high cell densities and multi-material printing. Cell viability typically reaches 80–95% under optimised conditions. Resolution: 100–500 micrometres.
Best suited to tissue engineering labs, biotech startups prototyping organ models, and university research groups needing high cell densities or multi-material scaffolds.
Inkjet (Droplet-Based) Bioprinting
Uses thermal or piezoelectric actuators to eject picoliter-volume droplets. Offers high speed (up to 10,000 droplets per second) and good cell viability (74–90%), but is limited to low-viscosity bioinks below 15 mPa·s. Resolution: 20–100 micrometres.
A natural fit for pharmaceutical R&D teams, drug discovery labs, and academic groups working on cell patterning, biosensors, or skin printing at speed.
Laser-Assisted Bioprinting (LAB/LIFT)
A pulsed laser vaporises a thin absorbing layer to propel bioink droplets onto a substrate. Completely nozzle-free, achieving the highest resolution (5–50 µm) and highest viability (above 95%) of any modality. Limited by expensive equipment and scalability constraints.
Reserved largely for advanced research institutes and well-funded biotech R&D centres focused on single-cell deposition, microvasculature, or high-precision tissue interfaces.
SLA/DLP-Based Bioprinting
Patterned light crosslinks photosensitive bioinks. Achieves 25–100 µm resolution with fabrication rates orders of magnitude faster than extrusion. Modern 2026 platforms use visible blue light (405 nm) with biocompatible photoinitiators like LAP to reduce genotoxic risk.
Favoured by biofabrication labs, regenerative medicine startups, and research groups printing geometrically complex constructs such as vascularised scaffolds or organ-on-chip platforms.
What Is Bioink? Types and Composition

Bioink is a printable formulation of living cells suspended in a biomaterial carrier, designed to form stable 3D structures while maintaining cell viability and function. It falls into two main categories: natural hydrogels such as alginate, gelatin, collagen, and silk, and synthetic polymers like PCL, PEG, and Pluronic. Selection depends on tissue type, printing method, required cell viability, and the mechanical strength needed for the final construct.
Bioinks must solve what researchers call the biofabrication paradox: materials mechanically strong enough to hold 3D shapes often inhibit cell migration, while materials cells thrive in are often too weak to maintain structure.
Natural Hydrogels
- Alginate: Derived from brown algae and crosslinked rapidly with calcium chloride, alginate is the workhorse bioink for early-stage tissue engineering and student lab work. Its lack of inherent cell adhesion sites limits its use in mature tissue constructs.
- GelMA: The most versatile single-component bioink in the field, GelMA is favoured by academic biofabrication labs printing skin, cartilage, vascularised tissue, and organ-on-chip constructs. Built-in cell adhesion and UV photocrosslinking make it the default starting point for most research groups.
- Collagen Type I: The most abundant protein in the human extracellular matrix, collagen is the bioink of choice for soft-tissue and FRESH-printed constructs in regenerative medicine and skin-printing research; biocompatibility outweighs its weak mechanical strength.
- Silk Fibroin: A cost-disruptive bioink developed by Indian institutions including IIT Guwahati, whose Muga silk formulations run roughly ₹2 per 10g against ₹10,000 for purified collagen. A practical fit for Indian academic labs and biotech startups working under materials-budget constraints.
Synthetic Polymers
- PCL (Polycaprolactone): A rigid, melt-extruded polymer used as a structural scaffold rather than a cell carrier. Standard in bone, cartilage, and load-bearing tissue research, where the construct must hold its shape across the 1–2 years it takes to degrade.
- PEG/PEGDA: A tunable photocrosslinkable matrix favoured by labs running fundamental cell-mechanics studies and drug-screening platforms, where mechanical precision matters more than native biocompatibility; peptide functionalisation is required for cell adhesion.
- Pluronic F-127: The most widely used sacrificial ink in the field: printed, then washed out to leave perfusable vascular channels behind. A staple in any lab working on vascularised tissue constructs or organ-on-chip platforms.
Decellularised ECM (dECM) Bioinks
Decellularised Extracellular Matrix (dECM) represents the most biologically instructive option for bioprinting. By removing the cellular components of donor organs while retaining tissue-specific growth factors and collagens, these bioinks create a “home” for new cells that perfectly mimics their natural environment.
- Liver dECM: Specifically promotes hepatocyte (liver cell) function.
- Cardiac dECM: Supports the maturation of cardiomyocytes (heart muscle cells).
- Corneal dECM: Currently being pioneered at IIT Hyderabad for ocular tissue engineering.
Real-World Applications of 3D Bioprinting in 2026
3D Bioprinting in 2026 spans five major domains: tissue engineering and organ scaffolds, drug testing and disease modelling, personalised medicine, bioprinted skin and wound care, and food bioprinting. Key advances include corneas in human trials, FDA-cleared cranial implants, organ-on-chip systems used across 150+ labs, and regulatory approval for cell-cultured meat. Among these, tissue engineering and drug testing are the most clinically and commercially advanced.
Tissue Engineering and Organ Scaffolds

Precise Bio achieved the world’s first transplant of a 3D-bioprinted functional cornea on 29 October 2025, at Rambam Medical Centre in Israel. A single donated cornea can potentially be expanded into approximately 300 printed implants, directly addressing the global shortage where only one donor cornea exists for every 70 patients who need one. Phase 1 trial results are expected in H2 2026.
Separately, 3DBio Therapeutics’ AuriNovo, a 3D-bioprinted living ear implant, continues in its Phase 1/2a trial since June 2022. In April 2024, 3D Systems received FDA 510(k) clearance for the world’s first additively manufactured PEEK cranial implant.
Drug Testing and Disease Modelling
Emulate’s Liver-Chip has demonstrated 87% sensitivity and 100% specificity for predicting drug-induced liver injury, now deployed in over 150 laboratories. The FDA Modernisation Act 2.0 (December 2022) removed the mandate for animal testing, explicitly permitting alternatives, including cell-based assays and organs-on-chips.
The Future: Will We 3D Print Full Organs?

Not soon, and not uniformly across all organs. 3D Bioprinting is already delivering simple avascular tissues (skin grafts, cartilage, corneal implants) into early clinical use, but full solid organs with native-scale vasculature remain a research problem rather than a manufacturing one. The gap is defined by two hard technical ceilings that the field has not yet been able to cross.
The first is the capillary gap. Printed perfusable channels currently floor at around 100 µm, while native capillaries operate at 5–10 µm. Until printing resolution closes that order-of-magnitude gap, dense constructs cannot be kept alive at organ scale.
The second is cell supply. A human liver contains roughly 100 billion hepatocytes; current iPSC bioreactors produce around 4 billion cells per 1-litre vessel. Scaling cell manufacturing to organ-relevant volumes is a parallel biomanufacturing problem that bioprinting alone cannot solve.
Progress is therefore expected to arrive incrementally and unevenly: thicker vascularised tissue patches and partial-organ constructs will likely reach early trials before any full solid organ does, and the order will depend on which tissue type’s vascular and cellular demands are cleared first.
FAQs
Can we 3D print a full human organ?
Not yet. Simple tissues like corneal implants and ear cartilage are entering clinical trials in 2025–2026. Full solid organs with complete vasculature are projected for 2035–2040 at the earliest, limited primarily by the capillary-scale vascularisation challenge.
Is 3D bioprinting used in drug testing?
Yes, and this is one of its most commercially mature applications. Bioprinted organ-on-a-chip models test drug efficacy and toxicity using human tissue constructs. The FDA Modernisation Act 2.0 (December 2022) removed the animal testing mandate, accelerating adoption.
What is happening with 3D bioprinting in India?
India has a growing ecosystem: IIT Guwahati’s Muga silk bioinks, IIT Hyderabad’s bioprinted corneas, AMTZ’s dedicated bioprinting facility, and startups like Pandorum Technologies, NBIL, and Avay Biosciences.
How much does a 3D bioprinter cost?
Entry-level research bioprinters start at ~$10,000–$20,000. Professional multi-printhead systems range from $50,000 to over $200,000. India-made alternatives like the MITO Plus aim to reduce costs. Indian bioprinters will generally start from around Rs. 8-10 Lakhs and can go upwards of Rs. 50 Lakhs as well.
About Manufactur3D Magazine: Manufactur3D is an online magazine on 3D printing. which publishes the latest 3D printing news, insights and analysis from all around the world. Visit our 3D Printing Education page to read more such informative articles. To stay up-to-date about the latest happenings in the 3D printing world, follow us on Facebook, LinkedIn and Twitter.